
Urethral Diverticulum
Incidence and Cause

A urethral diverticulum is an ‘outpouch’ of the urethra (waterpipe). This is a rare condition and only 150-200 cases are diagnosed in the United Kingdom each year.
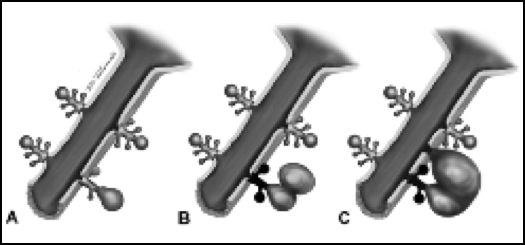
The cause of urethral diverticulae is not well understood. They are believed to develop from the Glands of Skene, which lubricate the lining of the urethra. Sequential obstruction and infection results in the gland expanding within the confines of the fascia tissues that surround the urethra. As such, the diverticulum tends to wrap around the urethra as it expands.
Urethral diverticulae are more commonly found in Afro-Caribbean women and were originally thought to be a consequence of childbirth, catheterisation or urethral (incontinence) surgery. It is now recognized that many urethral diverticulae (20%) occur in women that have never had children.
Symptoms and signs
Urethral diverticula are often asymptomatic and symptoms that are present tend to be non-specific. As such urethral diverticulae are difficult to diagnosis and the average delay between presenting symptoms and diagnosis is over 4 years! Classical teaching is that urethral diverticulae present with a triad of symptoms called the ‘three Ds’- Dysuria (painful micturition)
- Dyspareunia (painful sex)
- Dribble
- Urethral discharge
- Recurrent urinary tract infection
- Frequency/urgency
- Urethral pain
- Voiding dysfunction (retention)
Urethral diverticulae are associated with urethral cancer. The risk of cancer development is between 1-8%. The diagnosis is usually made when the diverticulum is removed.
Diagnostics
Diagnosis can be made by clinical examination of the vagina in half of cases. At LUS we have specialist Urologists who will examine you with a nurse chaperone present. Diagnosis is made using a combination of MRI scanning which gives the most accurate assessment of your pelvic (urethra) anatomy and video urodynamics, which assess your bladder and urethra function.
MRI scan showing the urethral diverticulum (white) wraps around the urethra in a horseshoe configuration

Video-urodynamics showing the urethral diverticulum as an ‘out-pouch’ of the urethra. Urinary incontinence is shown when the patient coughs
Treatment options
Surgery
Urethral diverticulum can be managed conservatively if they are asymptomatic, but most experts recommend that they are removed due to the (small) risk of cancer development The surgery to remove the urethral diverticulum is called urethral diverticulectomy and often combined with Martius fat pad interposition.
The urethral diverticulum is removed through an incision in the vagina. The defect in the urethra (waterpipe) is closed then closed (urethroplasty)
Urine (water) can find a route through the smallest of defects so in order to reduce the risk of the repair failing a flap of fat from one of your labia is tunnelled between the bladder and vagina repairs to form an interposition layer between the two lines of stitches. This is called a Martius fat pad.
A urethral catheter is left in place for 3-4 weeks to give time for the urethra to heal. The catheter drains into a collection bag on tour thigh. After this time a Cystogram dye X-ray is performed to check that the urethra is healed and the catheter is then removed.
The main risk of urethral diverticulectomy surgery is cough incontinence. In 10-30% of patients a second surgery is required to correct this problem. See section on Cough (Stress) Incontinence. Your LUS specialist will give more details of the surgery
More information about urethral diverticulectomy can be found via the BAUS leaflets and downloading the leaflet on removal of a diverticulum (outpouching) from the urethra