
Vesico-vaginal Fistula
Incidence and Cause
A vesico-vaginal fistula is an abnormal connection (a hole) between your bladder and vagina, which allows the continuous leakage of urine through the vagina. Vesico-vaginal fistulae are a common complication of childbirth in the developing world due to prolonged childbirth. This causes pressure on the pelvic floor and tissue necrosis (tissue death) of the back wall of the bladder and / or urethra (water-pipe). In sub-Sahara Africa 50-100,000 new cases occur every year, and 500,000 cases go untreated worldwide. Vesico-vaginal fistulae are rare In the Western world with modern gynaecology and obstetric practises. Only 100-150 cases of fistula occur in the UK each year although the number of cases is increasing. Nearly all vesico-vaginal fistulae occur because of surgical intervention. The vast majority in the UK occur following hysterectomy or Caesarean section, with an incidence rate of 0.3-2%. Other causes include:- Delayed labour (childbirth) in developing countries
- Hysterectomy
- Emergency Caesarean section
- Complex incontinence surgery
- Radiotherapy for pelvic cancer
- Infection
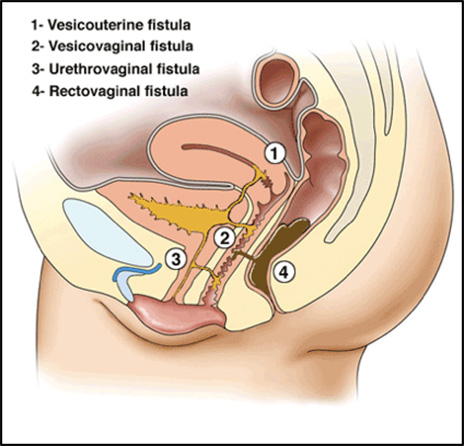
Fistula (holes) can occur between the bladder and vagina or more rarely between bladder and uterus or urethra (water-pipe).
In very rare cases fistula can also occur between the bowel and vagina.
Symptoms and signs
Bladder injury is sometimes recognised at the time of the initial surgery but on some occasions the hole develops later (days to weeks). This is a result of impaired blood supply and tissue necrosis (death), which causes tissue breakdown, leaving a hole. In cases where radiotherapy is involved fistulae may develop many years after the initial treatment. Fistula causes continuous leaking of urine through the vagina. In addition to the medical effects of urine leakage, vesico-vaginal fistulae cause huge emotional distress, and social isolation.Diagnosis
Diagnosis is usually made by clinical examination of the vagina. Radiological imaging is required to further assess the position of the fistula. This was previously done using X-rays but is now mostly commonly performed by MRI scanning to assess the bladder, and CT scanning to ensure that the ureters (draining the kidneys to the bladder) are not involved.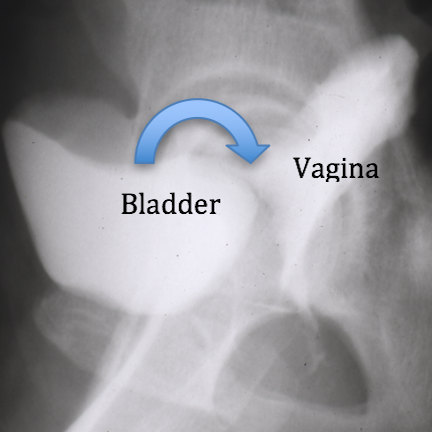
Fig 1 – Cystogram – X-ray showing dye leaking from bladder into vagina
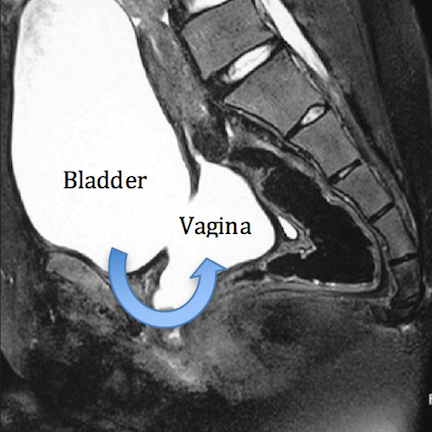
Fig 2 – MRI – Water (urine) shows up white. Bladder and the vagina behind both filled with urine
Treatment options
Catheterisation
A catheter is a small tube made of silicone or latex, which passes through your urethra (water-pipe) to keep the bladder empty and give the bladder a chance to heal. Occasionally, a vesico-vaginal fistula can heal by itself if a catheter is left in for several weeks.Surgical Repair
If the vesico-vaginal fistula is recognised early after surgery and the original surgery uncomplicated, then the fistula can sometimes be repaired early, within the first days. In most cases this is not the case. In such circumstances it is important that time is allowed for the tissue swelling and inflammation to be allowed to settle before a further surgical procedure is performed. Most specialists advocate a wait of at least 12 weeks (3 months) before surgical repair is performed. Vesico-vaginal repair can be performed through the vagina or through the abdomen. The success rates are generally equivalent (the same) for both approaches.Vaginal Repair of vesico-vaginal fistulae
If the fistula defect is accessible (can be reached) through the vagina then this is often the preferred route as it avoids another operation through tour abdomen (stomach). The bladder and vagina are separated to allow each to be sewn closed individually.
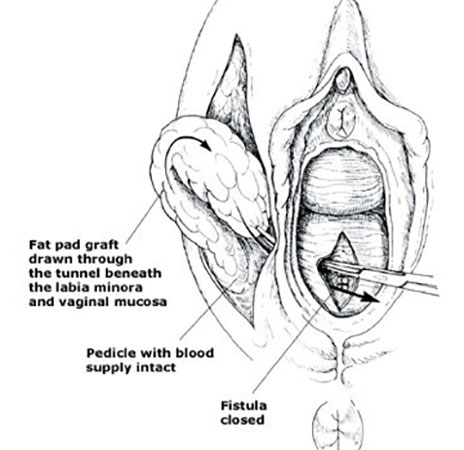
Urine (water) can find a route through the smallest of defects so in order to reduce the risk of the repair failing a flap of fat from one of your labia is tunnelled between the bladder and vagina repairs to form an interposition layer between the two lines of stitches. This is called a Martius fat pad.
Abdominal Repair of vesico-vaginal fistulae

V- vagina
If the fistula defect cannot be reached through the vagina, the defect is too large, or the ureter (kidney) drainage is affected then the operation can be performed through the abdomen (stomach). This is usually performed through a Bikini line (Pfannensteil) incision.
The bladder and vagina are separated to allow each to be sewn closed individually. In abdominal repairs fat from your stomach – Omental interposition (1) and (3)– is brought down to separate the bladder and vagina layers.
Following both vaginal and abdominal repairs a urethral and or abdominal catheter is left in place for 3-4 weeks to give time for the fistula to heal. The catheters drain into a collection bag on tour thigh. After this time a Cystogram dye X-ray (see above) is performed to check that the fistula is healed and the catheter is then removed.
More information about vaginal and abdominal repairs of vesico-vaginal fistulae can be found via the BAUS leaflets at https://www.baus.org.uk/patients/information_leaflets/category/3/bladder_procedures and downloading the leaflets Vaginal and Abdominal Repair of a Fistula between the Bladder and Vagina.