
Vaginal Prolapse
In women, the pelvic organs; the bladder at the front, the uterus, or womb in the middle and the bowel at the back are held in place by the muscles, tissues and ligaments in the pelvis which together constitute the pelvic floor support. Prolapse occurs when these supporting muscles, tissues and ligaments become weaker and are unable to hold the pelvic organs in place. Uro-genital prolapse is defined as the symptomatic descent of one or more of:- The front (bladder) vaginal wall
- The back (bowel) vaginal wall
- The apex (top) of the vagina (cervix/uterus) or vault (cuff) after hysterectomy
- First degree prolapse – when the uterus descends partially down into the vagina
- Second degree prolapse – when the uterus reaches the opening of the vagina
- Third degree prolapse – when the uterus sticks partially outside of the vagina
- Complete Procidentia – when the entire uterus descends below (outside) the vagina
Causes Of Prolapse
There are a number of factors, which contribute to the development of pelvic floor prolapse. The most common factors commonly associated with causing a prolapsed bladder are:- Childbirth: The most common cause. The weight of the developing baby on the pelvic floor and the vaginal delivery process stretch the pelvis floor muscles and support structures which prevent bladder, bowel and bowel prolapse
- Prior hysterectomy increases the risks of prolapse
- Excess Weight/Obesity
- Pelvic floor Straining: lifting heavy products, straining during bowel movement and long-term constipation can cause damage to the muscles of the pelvis floor
- Menopause: Oestrogen, the hormone, which maintains the strength of the vaginal muscles, is no longer produced after menopause, causing the pelvic floor to weaken. Tissue strength has a genetic component and pelvic floor weakness can run in families
Prolapse Symptoms
Some women experience no symptoms and the condition is only discovered when they are examined internally for other reasons. However, most women will experience symptoms, including:- The feeling that something has dropped down below, often described as a‘dragging sensation’
- Pelvic pressure and /or lower back pain
- Bladder Symptoms: Urinary frequency and a feeling that the bladder is not empty after urinating
- Bowel Symptoms: Difficulty emptying the bowels, and sometimes associated with altered bowel control
- Sexual Symptoms: Difficulty with sexual intercourse
- Recurrent urinary tract infections
Prolapse Diagnosis

Sims Speculum Examination
Your consultant will examine your abdomen and vagina using a retractor called a speculum. This examination is not painful.
A nurse chaperone will be present during this examination.

Severity of Prolapse
Uro-genital prolapse is measured using the POPQ or Baden Walker systems where the amount of descent is measured relative to the vaginal opening
The consultant will also assess the strength of your pelvic floor (pelvic floor tone)
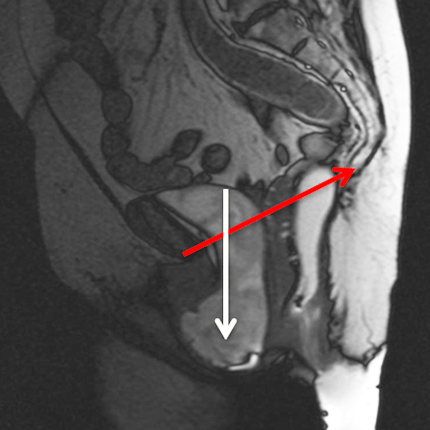
Strain or defecating MRI scan
An MRI scan can also be performed to look at your pelvic floor anatomy in more detail. The MRI scan takes approximately 30 minutes and is not painful.
Your consultant will give further details.
MRI picture showing bladder prolapse through the pelvic floor (shown in white below red line.
Prolapse Treatment
Grade 1 prolapse that produces no pain or discomfort usually requires no medical or surgical treatment. However, your consultant may recommend you avoid lifting or straining.
Pelvic Floor Exercises

Pelvic floor exercises help improve the tone (strengthen) the muscles of the pelvic floor. This helps to support the bladder and tighten around the bladder neck and urethra (water-pipe) during times of increased abdominal pressure (eg bending or running). Specific exercise can be taught to try and tighten the muscle. These exercises can be augmented by the use of vaginal cones (weights), biofeedback monitors or electrical stimulation. Pelvic floor exercises are taught by physiotherapists and need to be practised regularly at home to be effective. Pelvic floor exercises can improve stress incontinence in up to 70% of women, but only work if the exercises are continued.
More information about pelvic Floor Exercises can be found via the BAUS leaflets at https://www.baus.org.uk/patients/information_leaflets/category/3/bladder_procedures and downloading the leaflet on Pelvic Floor Exercises (in women).
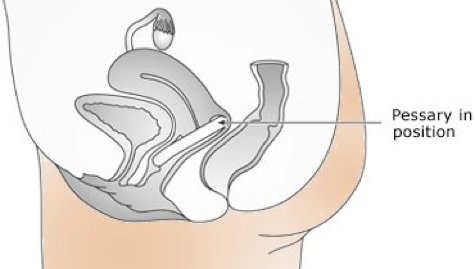
Vaginal Pessaries
Pessaries are rubber rings, similar to contraceptive diaphragms, which are inserted into the vagina to lift the bladder or uterus. Vaginal pessaries can be used by patients who would like to avoid surgery, or have health problems that make the risks of surgery too great. In some patients, a short trial with a pessary may demonstrate whether bladder or bowel symptoms will improve with the prolapse corrected, and whether surgery is indicated.
There are many different pessary shapes and sizes to meet patient’s individual anatomy support.
Our specialist nurses and physiotherapists will fit you for a pessary appropriate to your needs. If a pessary fits well and is comfortable, then over half continue to use it successfully on a long-term basis.
Pessaries are commonly combined with a vaginal estrogen cream to keep the vaginal lining lubricated and healthy.
Vaginal pessaries can cause local irritation and discharge. Poorly fitting pessaries can cause vaginal bleeding or erosions.
Surgery for Prolapse
There are a number of different operations for pelvic organ prolapse. The operations are broadly divided into procedures performed via a vaginal approach to tighten the vaginal tissues from below. For patients with more significant prolapse of the vaginal vault abdominal procedures can be performed to lift the pelvic organs and secure them above pelvic floor using mesh or non-mesh suture techniques.Abdominal surgery
- Non-mesh (autologous) sacrocolpopexy / sacrocolpopexy A strip of the abdominal wall is used instead of mesh to attach the top of the vagina or uterus to the ligaments on the front of the sacrum (tailbone). This offers women an alternative to the use of synthetic mesh (see Mesh Complications for discussion of mesh risks)
- Mesh sacrocolpopexy / sacrocolpopexy An abdominal mesh is implanted to attach the top of the vagina or uterus to the ligaments on the front of the sacrum (tailbone). This generally offers the best long-term support for women who have severe or recurrent prolapse (see Mesh Complications for discussion of mesh risks)
- Hysterectomy The LUS consultants work in conjunction with gynaecology colleagues. A hysterectomy can be considered if there are other reasons for the uterus to be removed. This operation removes the uterus or top portion of the uterus (leaving the cervix in place to connect support stitches too) The operation can be done vaginally, robotically, laparoscopic or abdominally – depending on the specific prolapse situation for the patient. When used to treat prolapse a concomitant procedures has to be done to prevent prolapse.
Vaginal Surgery
- Anterior colporrhaphy – cystocoele repair Anterior colporrhaphy is performed with stitches to recreate support of the anterior vaginal wall under the bladder and support the bladder like a shelf. Anterior colporrhaphy corrects a hernia or ballooning of a weak front wall of the vagina and often improves bladder emptying. The stitches dissolve after 6 weeks, relying on the tightened tissue to maintain support
- Posterior colporrhaphy – rectocoele repair Posterior colporrhaphy is performed with stitches to support the posterior vaginal wall between the vagina & lower colon/rectum. The weakened back wall of the vagina is tightened to give better strength. This procedure may help bowel evacuation and relief of pelvic pressure or low back pain. The stitches dissolve after 6 weeks, relying on the tightened tissue to maintain support
- Enterocoele repair An enterocoele repair is performed with dissolving stitches to close off the weak area which allows the small bowel to descend and bulge through the vagina
- Sacrospinous fixation This operation is a vaginal operation that supports the top of the vagina to deep pelvic ligaments with permanent stitches