
Painful bladder syndrome (PBS) and Interstitial Cystitis (IC)
Incidence
Painful bladder syndrome (PBS) also called chronic pelvic pain syndrome (CPPS) is defined as the occurrence of persistent or recurrent pain perceived in the urinary bladder region, accompanied by at least one other symptom, such as pain worsening with bladder filling and day-time and/or night-time urinary frequency. CPPS encompasses a wide variety of pain syndromes, which affect the organs of the pelvis including the bladder, the urethra, vagina, groin and prostate in men.
Inflammatory cystitis is a chronic inflammatory condition of the bladder wall (in the same way that rheumatoid arthritis is an inflammatory condition of joints). It is not caused by bacteria and will not respond to antibiotics. At the most severe end of the disease spectrum is Interstitial Cystitis (IC), where the inflammation is so severe that it causes ulceration of the bladder wall. True Interstitial Cystitis is rare and accounts for less than 10% of patients with inflammatory cystitis.
Reports of PBS prevalence have varied greatly, along with the diagnostic criteria and populations studied. Incidence ranges from 0.06% to 30%. There are no established differences in race or ethnicity. PBS affects women more often than men, with nine out of ten sufferers being female. Onset is typically after the age of 40, although it can occur at any age.
Causes
Patients with PBS / IC usually describe a specific date of onset. It is believed that an initial unidentified insult to the bladder, leads to damage of the bladder lining, and neurogenic inflammation and pain is thought to result.
One theory is that IC is an autoimmune response following a bladder infection. The infection and the body’s defence response to the infection, damage the lining of the bladder, allowing urinary toxins to infiltrate the bladder wall and set up an inflammatory reaction. The inflammatory reaction damages nerve endings, which become sensitised, and the pain worsens, independent of the initial infection. Although, often implicated as an initiating factor, no specific (bacterial) infection has as yet been implicated.
This is very different to standard cystitis, which is caused by a bacterial urinary tract infection and responds to antibiotics.
Another field of research has focused on the layer that coats the lining of the bladder called the glycocalyx. This consists mainly of substances called mucins and glycosaminoglycans (GAG). This layer normally protects the bladder wall from toxins within urine. Researchers have found that this protective layer of the bladder is “leaky” in about 70 per cent of IC patients. There is a theory that this may allow substances in urine to pass into the bladder wall where they might trigger the inflammatory reaction.
Symptoms and Signs
- The classical symptoms of PBS / IC are frequency, urgency and bladder (pelvic) pain
- In early or mild cases, the need to go to the toilet very frequently may be the only symptom. In the most severe cases, patients may need to go to the toilet up to 30 times (hourly or less) during a 24 hour period
- An urgent need to urinate frequently day and night. This is often associated with a decreased bladder capacity
- Pain, pressure and tenderness around the abdomen, bladder, urethra, vagina pelvis (prostate in men), and perineum
- A significant characteristic of PBS/IC is pain increases during bladder filling and is alleviated with urination (although when the bladder walls touch at the end of urinating the pain is often worsened)
- Pain is often made worse by sexual intercourse (ejaculation in men)
- Symptoms may worsen for women during menstruation
- Stress often worsens symptoms
Although symptoms often have a mild onset, they typically worsen rapidly with time and often with a cyclical pattern “relapse and remit”. The cycles of pain may vary from mild to severe and in the severe cases are debilitating. In some patients there is a ‘honeymoon period’ where symptoms improve for a period (usually weeks) following their acute onset, before returning to a similar pattern as before.
Symptoms can vary from day to day. If left untreated, PBS / IC can lead to reduced bladder capacity, bleeding from the bladder lining and more rarely bladder ulcers. In long standing cases scarring and stiffening of the bladder may make the bladder pressurised and result in urinary incontinence and kidney damage.
Diagnosis
PBS is a diagnosis based upon the symptom complex described by patients. Your consultant will take a detailed history of your symptoms. The severity of your symptoms can be categorised by specialist questionnaires called the O’Leary-Sant Symptom Index, also known as the Interstitial Cystitis Symptom Index (ICSI). These questionnaires can be downloaded from here.
It is important to exclude other disorders of the urinary system that may cause similar symptoms to PBS / IC. There are strict criteria, which define PBS and particularly IC, based on laboratory (urine) tests, imaging of the bladder and pelvis, urodynamics, which assess bladder function, cystoscopic visualisation of the bladder and biopsy of the bladder wall. Tests include:
- Urine analysis and culture
- In men, laboratory examination of prostate cells
- Imaging of the bladder, which may include ultrasound and possibly MRI to exclude structural abnormalities od the urological or gynaecological symptoms
- Video-urodynamic assessment to assess bladder function
- Cystoscopy and biopsy of the bladder wall
During cystoscopy the bladder is distended (stretched) in order to assess the inflammation in the bladder lining and capacity of the bladder. When inflammation is present, the bladder wall shows glomerulations (bladder haemorrhages). In severe cases (IC) the bladder lining is ulcerated. These are called Hunner’s lesions. The severity of inflammatory cystitis can then be categorised.
Bladder biopsies are performed to look for inflammatory cells. Mast cells are often seen in the bladder wall biopsy. These cells produce histamine, and an increased number is suggestive of inflammatory cystitis.

Glomerulations

Glomerulations bleeding as bladder empties

Hunner’s Ulcer

Classification of Inflammatory Cystitis
Treatment
Fortunately, there are very effective treatments for most patients with PBS / IC. Patients often respond to different treatment modalities and combinations, and treatment is individualised to the patient’s particular symptoms.
Diet
There is good evidence that dietary triggers/exacerbates PBS symptoms, although these are not predictable between individual patients. Common triggers are alcohol, tomatoes, spices, chocolate, caffeinated and citrus beverages. High-acid foods may contribute to bladder irritation and inflammation. Some people also note that their symptoms worsen after eating or drinking products containing artificial sweeteners. Eliminating various items from the diet and reintroducing them one at a time may determine which, if any, affect a person’s symptoms. However, maintaining a varied, well-balanced diet is important.
Behavioural Therapy and Acupuncture
Many patients are helped by bladder training and pelvic floor exercise regimes. Biofeedback can help patients monitor their response. In some patients pelvic floor trigger points may aggravate pain. Physical manipulation, acupuncture and electrical stimulation may help alleviate these triggers. Our nurse specialists are trained to treat and educate patients in these techniques.
The method of delivering impulses through the skin is called transcutaneous electrical nerve stimulation (TENS). With TENS, electrical stimulation is used on trigger points on the lower back, pubic area, perineum (between the legs) or using special devices into the vagina in women or into the rectum in men. Sessional treatment usually takes place on a weekly basis. Electrical pulses help strengthen pelvic muscles that help control the bladder, and trigger the release of substances that block pain.
Medication
The majority of PBS / IC patients can be managed, and their symptoms controlled by oral medication. Medications include anti-inflammatories and anti-histamines. For patients with more severe symptoms anti-depressants and anti-epileptic drugs can be used to dampen the nerve responses. These drugs are often used in combination and can be very effective treatments. These drugs should only be used under specialist advice.
Bladder Hydrodistension
Bladder distension or stretching is used for diagnosis and therapy of interstitial cystitis. Under a general anaesthetic, your Urologist fills the bladder with fluid and keeps it stretched for 1 minute. Reduced bladder capacity, glomerulations and bleeding are suggestive of inflammatory cystitis.
Bladder distension can be therapeutic. Many people find there is an improvement after the procedure. Researchers are not sure why distension helps, but some believe it may increase capacity and interfere with pain signals transmitted by nerves in the bladder. Symptoms may temporarily worsen 24 to 48 hours after distension, but should return to normal levels or improve within 2 to 4 weeks. About 30 per cent of patients report an improvement.
Bladder Instillations
During a bladder instillation, the bladder is filled with a drug solution via a catheter (narrow tube) that is then retained in the bladder for up to one hour before removal. The drugs are aimed at replenishing the glycosaminoglycans (GAG) layer, which protects the bladder lining. Several different bladder instillations are now available. Drugs that are used for bladder instillations include heparin, dimethyl sulfoxide (DMSO), sodium bicarbonate, hydrocortisone and local anaesthetics. Most people with PBS / IC who respond to bladder instillations notice an improvement in symptoms 3 or 4 weeks after the first 6 to 8-week cycle of treatments.
Instillations are usually repeated on a weekly cycle for 6 weeks and repeated, as needed depending on symptoms.
Neuromodulation
Percutaneous Nerve Stimulation and Sacral Nerve Stimulation
Electric stimulation can be used to neuromodulate (regulate) the nerves to the bladder. This can be accomplished either through the skin (percutaneous) or with an (sacral) implanted device.

Percutaneous tibial nerve stimulation (pTENS).
Your consultant will examine your abdomen and vagina using a retractor called a speculum. This examination is not painful.
In this case electrical stimulus is applied through acupuncture needles placed in the ankle. The needles stimulate the tibial nerve, which also supplies the bladder. pTENS is performed in 30 minute sessions weekly over 12 weeks.

Sacral Nerve Stimulation
The most recent development in electrical stimulation is implantation of sacral nerve stimulator (SNS). In this technique, the nerves to the bladder are directly stimulated through the sacrum in the lower back. An external test implant is worn for 3 weeks. Patients that have responded well in early trials are offered a permanent implant of a ‘bladder pacemaker’ implanted in the fat over the upper buttock.
Botox

Botox
Botulinum toxin can be injected into the bladder wall to block nerve endings and relax the bladder (Detrusor) muscle
However, over-paralysis of the bladder can lead to difficulty in passing urine. 1-5% (1 in 20) patients require to use in-out catheters temporarily until the Botox effect wears off
Surgery
Surgery should be considered only if all available treatments have failed and the pain is disabling. Surgical intervention for PBS and IC is complex, and should only be done by specialist surgeons with extensive experience of this work.
Fulguration and resection of ulcers
Fulguration involves burning bladder (Hunner’s) ulcers with electricity or a laser. When the area heals, the dead tissue and the ulcer fall off, leaving new, healthy tissue behind. Resection involves cutting around and removing the ulcers. Both treatments are done under anaesthesia and use special instruments inserted into the bladder through a cystoscope.
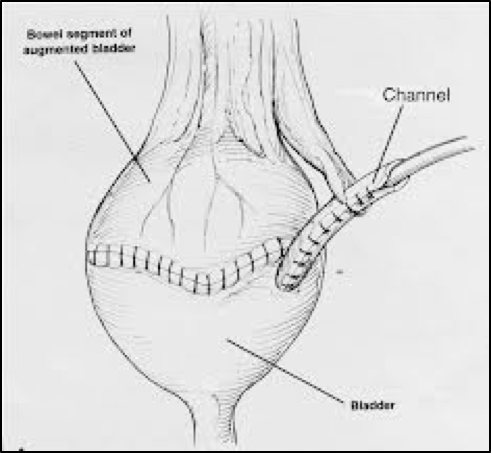
Bladder augmentation / substitution
This is a surgical treatment designed to make the bladder larger. The inflamed sections of the patient’s bladder are removed, leaving only the base of the bladder and healthy tissue. A piece of the patient’s colon is then removed, reshaped, and attached to what remains of the bladder. The augmented bladder has greater capacity, and the coordinated bladder contractions (spasms) are prevented. Most patients will have to catheterise to empty the augmented bladder. The effect on pain varies greatly; PBS can sometimes recur even after the bladder is removed.
Bladder removal (cystectomy)
This is a more rarely used surgical option, only suitable for the most severe and debilitating cases. Once the bladder has been removed, different methods can be used to reroute the urine.
A neobladder is formed from bowel refashioned into a pouch. This is then attached to the urethra so that the patient can empty by either abdominal pressure or in most cases catheterisation.
Mitrofanoff
For patients unable to catheterise through a painful urethra, a tube can be fashioned from appendix or bowel to empty the bladder through the umbilicus or abdominal wall. This is called a Mitrofanoff procedure. These are complex reconstructive surgeries for motivated patients. Only a few surgeons have the special training and expertise needed to perform these procedures.
A more simple diversion of urine is to attach the ureters to a piece of colon that opens onto the skin of the abdomen. This procedure is called a urostomy and the opening is called a stoma. Urine empties through the stoma into a bag attached to the abdominal wall under the clothing.
The European Association of Urology has issued guidance on treatment on PBS / IC. A summary of their treatment recommendations is shown below (from EAU Guidelines)
